



What is dysautonomia?
The autonomic nervous system (ANS) is the part of the nervous system that regulates functions that are automatic in nature such as heart rate, blood pressure, digestion, excretion, perspiration, temperature regulation, pupil dilation, circulation, and respiration among others.
The ANS is responsible for maintaining homeostasis, or equilibrium, in the body. When there is a dysfunction or failure of the autonomic nervous system, the result is a disorder classified as a type of dysautonomia. Dysautonomia is not a diagnosis. It’s an umbrella term to describe autonomic disorders. It’s sometimes referred to as autonomic dysfunction or autonomic neuropathy.
It is estimated that 70 million people worldwide have some form of autonomic dysfunction. Often dysautonomias are invisible illnesses. Patients may not look sick, and yet they have symptoms that make it difficult to work, go to school, and perform activities of daily living.
Common Symptoms
The symptoms experienced by dysautonomia patients vary based on the type of autonomic dysfunction and where the dysfunction is occurring within the body.
Here are the seven most common symptoms:
- Fatigue
- Brain Fog
- Lightheadedness (pre syncope)
- Body Temperature Dysregulation
- Difficulty with upright posture
- Palpitations
- GI Issues
Dysautonomia symptoms are not limited to these seven. The organ systems most commonly affected in dysautonomias are neurological, pulmonary, cardiovascular, urinary, gastrointestinal, secretomotor and pupillomotor. Because autonomic disorders affect multiple organ systems, the presentation of symptoms are heterogenous, widely varying between different individuals. For example, one patient with POTS (a common autonomic disorder) may have the chief complaint of abdominal pain while the next POTS patient identifies migraine headaches as their primary symptom.
Orthostatic Intolerance

One common sign of autonomic dysfunction is difficulty maintaining upright posture. This is known as orthostatic intolerance and involves abnormal blood pressure and heart rate. Patients with orthostatic intolerance present with feelings of lightheadedness, dizziness, and brain fog. It’s caused by a loss of blood flow to the brain, heart, and lungs. This is not a life-threatening decrease in blood flow, but it’s bothersome and some cases causes fainting.
Another symptom of orthostatic intolerance or orthostatic hypotension when standing upright is an annoying pain in the back of the neck and shoulders. This is not always a symptom nor a primary symptom. Because of the distribution of the discomfort, this is sometimes referred to as the “coat hanger sign” which occurs as pain in the back of the neck when standing. The exact mechanism of the coat hanger phenomenon is unknown, but one theory suggests it is a kind of cramp caused when the antigravity muscles holding up the head receive too little blood flow.
The following graphic depicts common symptoms and the organ systems affected.
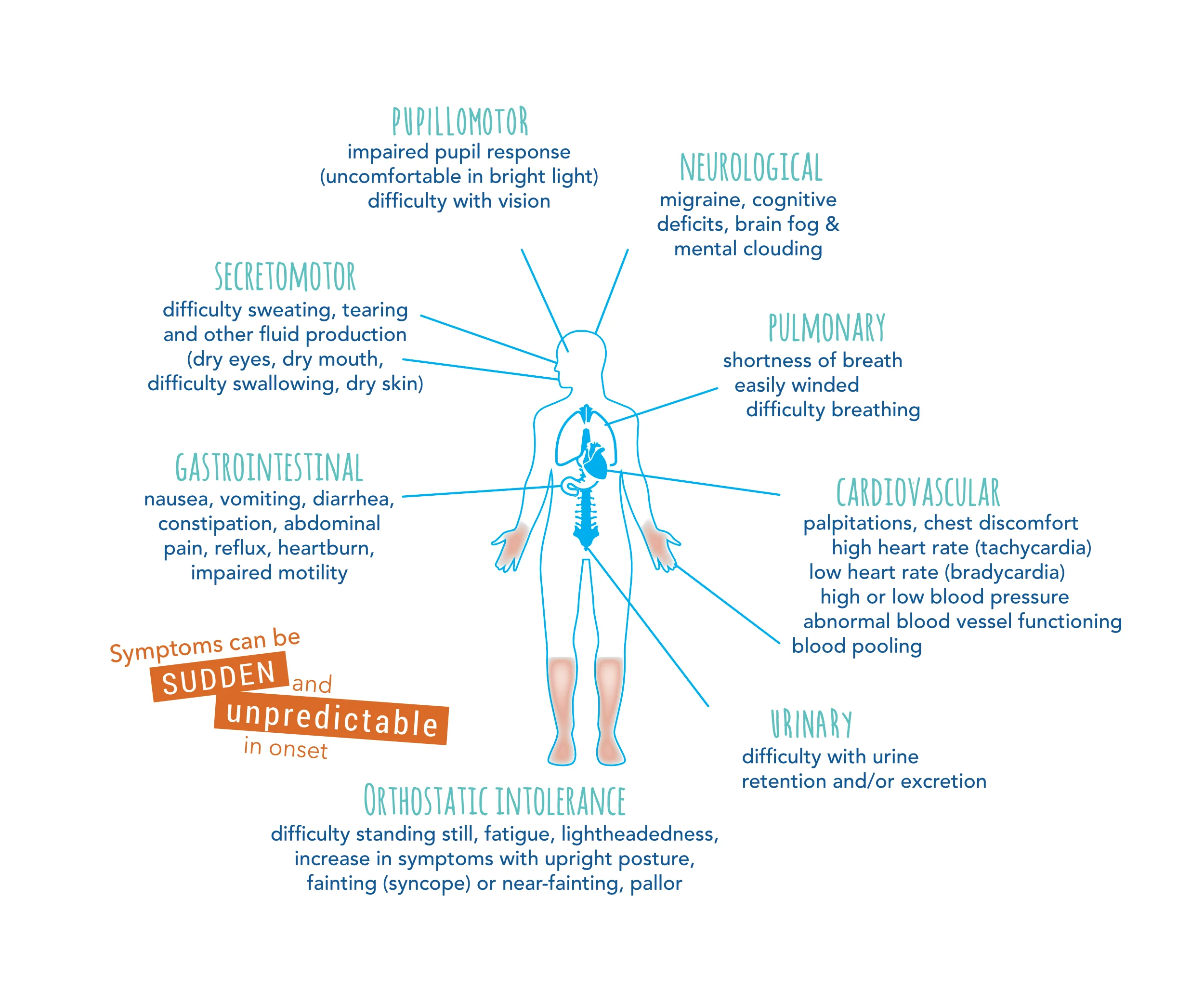
Pupillomotor Symptoms: impaired pupil response (uncomfortable in bright light) and impaired vision.
Neurological Symptoms: migraines, cognitive deficits, brain fog and mental clouding.
Pulmonary Symptoms: shortness of breath, easily winded, and difficulty breathing.
Cardiovascular Symptoms: palpitations, chest discomfort, high heart rate (tachycardia), low heart rate (bradycardia), high or low blood pressure, abnormal blood pressure functioning, and blood pooling.
Urinary Symptoms: difficulty with urine retention and/or excretion.
Gastrointestinal Symptoms: nausea, vomiting, diarrhea, constipation, abdominal pain, reflux, heartburn, and impaired motility
Secretomotor Symptoms: difficulty sweating, tearing, and other fluid production (dry eyes, dry mouth, difficulty swallowing, dry skin).
Orthostatic Intolerance Symptoms: difficulty standing still, fatigue, lightheadedness, increase in symptoms with upright posture, fainting (syncope) or near-fainting, and pallor.
Symptoms can be triggered by dehydration, tight clothing, hot environments, stress, and alcohol consumption.
Again, this is not an exhaustive list of symptoms. Any symptom in any organ system could potentially be the result of an autonomic disorder. Understanding which symptoms affect you the most is important when identifying treatments with your doctor. Once you’ve been diagnosed with an autonomic disorder, every future or co-existing condition needs to be considered in light of your diagnosis and considered as potentially being caused by the autonomic disorder.
Types of Dysautonomia
There are at least 15 distinct dysautonomias. The most common are postural orthostatic tachycardia syndrome (POTS) and neurocardiogenic syncope/autonomic mediated syncope.
Autonomic dysfunction can occur at any age: pediatric, adult, or geriatric. It can range from mild to disabling and may or may not be neurodegenerative. Because there are many forms of dysautonomia, we use the singular term “dysautonomia” to reference autonomic disorders in general or when referring to a specific condition such as “orthostatic hypotension.” We use “dysautonomias” when referring to many disorders of the autonomic nervous system.
Age and Onset of Dysautonomias
Pediatric Onset (very rare)
Also known as genetic or hereditary dysautonomias, these conditions often reflect problems or mutations which occur during the development of the autonomic nervous system. One type of mutation, found almost exclusively in people of Ashkenazi Jewish heritage, affects the autonomic and sensory nervous system development causing familial dysautonomia (FD)
Another mutation causes an increased level of phenylalanine (Phe) in the bloodstream resulting in a metabolic disorder called phenylketonuria (PKU). Another mutation in the ATP7A gene that is responsible for transporting copper throughout the body causes “kinky hair” and is known as Menkes disease. In Hirschsprung’s disease there is a lack of development of nerve cells in the enteric nervous system. It’s important to note that, in general, dysautonomias in early childhood are rare. For more information: Pediatric Dysautonomias.

Other pediatric autonomic disorders include:
Hereditary Sensory and Autonomic Neuropathy (HSAN)
Congenital Central Hypoventilation Syndrome (CCHS)
Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT)
Teen/Adult Onset
In teens and adults, autonomic dysfunction usually reflects functional changes in a generally intact autonomic nervous system. It is estimated that postural orthostatic tachycardia syndrome (POTS), a common autonomic disorder, affects 1 out of every 100 teens. Dysautonomias in adults often are associated with, and may be secondary to, another disease process or a drug. Common secondary causes include medications, chemotherapy, radiation treatments, spinal cord or head injury, or diabetes (such as diabetic autonomic neuropathy). Less commonly, the body’s immune system mistakenly attacks and damages certain parts of the autonomic nervous system in autoimmune autonomic ganglionopathy.
Autonomically mediated syncope, also called vasovagal syncope, neurally mediated syncope or neurocardiogenic syncope, is another example of teen/adult dysautonomia. Individuals with autonomically mediated syncope suffer from frequent episodes of fainting or near fainting where the blood pressure drops by 20 mmHg systolic/ 10 mmHg diastolic with upright posture. Most patients have symptoms with little change in heart rate. In some cases, the drop in blood pressure occurs as a compensatory function following tachycardia, as seen in POTS, or bradycardia can precede a drop in blood pressure. For more information: Teen and Adult Onset of Dysautonomia.
The most common form of dysautonomia is Postural Orthostatic Tachycardia Syndrome (POTS).
Dysautonomias Ages 50+
Any autonomic disorder diagnosis after the age of 50 is considered geriatric onset. In these patients, dysautonomia typically reflects a neurodegenerative disease. The degeneration may be in the form of lesions in the central nervous system, as in multiple system atrophy (MSA), or in loss of autonomic nerves not involving the central nervous system, as in pure autonomic failure (PAF). Most geriatric cases involve damage to nerves that result in loss of autonomic reflexes, also known as autonomic failure. It is common in geriatric patients to experience some orthostatic hypotension which is characterized by a drop in blood pressure upon standing.
Neurogenic orthostatic hypotension is a neurodegenerative form of dysautonomia in which the autonomic system loses the ability to properly regulate blood pressure as one moves from sitting or lying down to standing. Evidence suggests that the autonomic nervous system (ANS) is affected by dementia. In many types of dementia, neuropathological lesions can be found in the ANS. Lewy body disorders (LBD), which include Parkinson’s disease (PD) and dementia with Lewy bodies (DLB), commonly involve ANS dysfunction.
For more information: Dysautonomias Ages 50+
Primary, Secondary or Idiopathic
Regardless of when an autonomic dysfunction occurs in life, these disorders can be primary, secondary, or idiopathic. A primary dysautonomia is when we know autonomic dysfunction is the main disease process. Examples of primary dysautonomias include familial dysautonomia, multiple system atrophy, pure autonomic failure, and some forms of syncope among others.
Secondary dysautonomias are experienced because of another disease process, as in autonomic neuropathy associated with diabetes or POTS resulting from an autoimmune disease.
Conditions in which secondary dysautonomia might occur:
Amyloidosis
Celiac disease
Charcot-Marie-Tooth disease
Chiari malformation
Crohn’s disease
Ehlers-Danlos syndrome
Ulcerative Colitis
Guillain-Barre syndrome
Human immunodeficiency virus (HIV)
Lambert-Eaton syndrome
Lupus
Lyme disease
Muscular sclerosis
Parkinson’s
Rheumatoid arthritis
Sarcoidosis
Sjogren’s syndrome
Vitamin B and E deficiencies
Diabetes
Idiopathic dysautonomias are autonomic nervous system disorders where the main disease process is unknown. The pathophysiology of most autonomic disorders is complex and not well known, therefore it is helpful to discuss with your doctor if your dysautonomia is a primary, secondary, or idiopathic disorder. You may not be able to get to the root of your dysautonomia, but the process of trying to identify the cause may help with symptom treatment and management.
Coexisting Conditions and Autonomic Symptoms
Since dysautonomia patients experience many symptoms from multiple organ systems, it is helpful to consider the possibility of underlying causes or coexisting conditions.

Common coexisting conditions associated with autonomic disorders:
| Coexisting Conditions | Autonomic Symptoms |
|---|---|
|
Autoimmune Autonomic Ganglionpathy (AAG) (Considered both an autoimmune and autonomic disorder) |
Orthostatic hypotension (OH), gastrointestinal issues, urinary retention |
|
Autoimmune Encephalopathy |
Excessive sweating, labile blood pressure and heart rate |
|
Autoimmunity |
Dry eyes, dry mouth, dilated pupils, joint pain, swollen lymph nodes. |
|
Celiac Disease |
Gastrointestinal issues |
|
Charcot-Marie Tooth Disease |
ogressive foot drop, imbalance, sensory loss, gait abnormalities, autonomic neuropathy, abnormal heart rhythms, and difficulty breathing |
|
Chiari Malformation |
Neck pain, balance problems, numbness in the arms and legs, ringing in the ears, headache made worse by coughing or straining |
|
Chronic Regional Pain Syndrome |
Constant burning pain, pain that is disproportionate (more than what it should be), one limb that is or has experienced pain and swelling with or without trauma |
|
Diabetes |
Chronic pain in feet, urinary problems, erectile problems in males |
|
Guillain-Barre Syndrome |
Labile blood pressure and heart rate, constipation |
|
Hybermobile Ehlers Danlos Syndrome (EDS) |
Hypermobile joints, history of multiple dislocated joints, stretchy skin, very thin skin |
|
Intercranial Hypertension |
Cerebral fluid imbalance causing dizziness, nausea, neck pain, sleep disturbances, headaches, flushing, vision changes, fainting |
|
Mast Cell Activation Syndrome |
Flushing (dry, hot, red face or upper body), multiple hypersensitivities, hives, anaphylaxis |
|
Median Arcuate Ligament Syndrome |
Pain in the upper middle stomach area after eating, exercising, or shifting body position, bloating |
|
Paraneoplastic Autonomic Neuropathy |
Gastroparesis, orthostatic hypotension (OH) |
|
Parkinson’s Disease |
Orthostatic hypotension (OH), sexual dysfunction, swallowing or gastrointestinal disorders, bowel and bladder abnormalities, and sleep disturbance |
|
Sjogren’s Disease |
Dry eyes and dry mouth, fatigue, orthostatic tachycardia |
|
Sleep Disorders |
Difficulty staying awake, difficulty sleeping, commonly experience unrefreshed sleep |
|
Small Fiber Neuropathy |
Pins and needles, burning and/or numb sensations of extremities, especially at rest |
|
Systemic Lupus Erythematosus (SLE) |
Skin rashes, paresthesia, fatigue |
Diagnosing Dysautonomias
Clinical Assessment: A doctor who understands dysautonomia should conduct a clinical assessment which includes a comprehensive medical history and physical examination.
Active Stand Test: This test (also known as an orthostatic vitals test) can be performed in a doctor’s office by a nurse or properly trained staff member. The test results may provide meaningful data about the patient’s response to orthostatic stress. More importantly, an orthostatic vitals test may confirm a suspected dysautonomia without the use of expensive diagnostic testing.
Tilt Table Test: This test is done to see how the body reacts to changes in position, specifically if standing up (orthostasis) provokes orthostatic hypotension, neurally mediated hypotension, an excessive increase in pulse rate, or autonomically mediates syncope. The tilt table test used to be considered the “gold standard” in testing for dysautonomias. Today, most clinicians are comfortable confirming an autonomic disorder with active stand test.
Other tests available at many major autonomic laboratories include:
Quantitative Sudomotor Axon Reflex Test (QSART)
The Valsalva Maneuver
The Cold Pressor Test
Heart Rate Variability
Blood Volume Testing
Catecholamine Tests
Antibody Test
Skin Biopsies
For more information on clinical autonomic testing see our course Introduction to Clinicial Autonomic Testing or the Autonomic Testing Table resource.

Treating Dysautonomia
There is no known cure for autonomic disorders, but the symptoms can be managed. Any treatment should be done while under the care of a provider who understands dysautonomias. Some of the treatments used for common symptoms include:
- Increasing water intake by 2-3 liters of fluid daily to keep your blood volume up. Discuss the amount of fluid intake with your provider.
- Adding sodium (salt) to your daily intake. Salt helps to retain fluid volume in your blood vessels which helps with blood pressure. In most cases, 5-9 grams of salt daily. Discuss with your provider.
- Exercise
Non-Pharmacological Treatments
Several non-pharmacological treatments are used to help patients with autonomic disorders. Although these treatments do not involve medicine, patients should discuss the use of such therapies with their provider as a part of their treatment plan.
Top 10 Non-Pharmacological Treatments
| Treatment | Helps with | Notes for Health Clinicians |
|---|---|---|
|
Education |
Promotes self-management and adherence through understanding of triggers and physiology |
Ensure patients understand the rationale behind each intervention; pair education with written plans and follow-up reinforcement |
|
Exercise & Movement |
Improves cardiac output, vascular tone, and muscle pump activity; reduces deconditioning and venous pooling |
Use graded, recumbent protocols; tailor for comorbidities like EDS or ME/CFS; monitor HR goals in POTS; avoid wheelchairs unless absolutely necessary |
|
Fluids |
Expands plasma volume, increases preload, and reduces reflex tachycardia via volume buffering |
Recommend 2–4L/day; space throughout the day; consider electrolyte solutions for patients with GI symptoms |
|
Salt Intake |
Enhances fluid retention and sympathetic vasoconstriction; supports cerebral autoregulation |
Up to 10g/day as tolerated; avoid in CHF/CKD; can be paired with fludrocortisone in resistant cases |
|
Avoiding Heat |
Prevents peripheral vasodilation and exacerbation of orthostatic hypotension |
Advise cool showers, no saunas/hot tubs, and temperature regulation techniques; morning is the highest risk period |
|
Compression Garments |
Supports venous return by reducing lower extremity and abdominal blood pooling |
Use 30–40 mmHg waist-high stockings and step-in abdominal binders; remove during rest; helpful for travel or long standing |
|
Small, Frequent Meals |
Reduces postprandial splanchnic vasodilation that leads to hypotension and GI pooling |
Avoid large meals, refined sugars, and high-fat content; consider low-residue or liquid diets in patients with GI symptoms or gastroparesis |
|
Countermaneuvers and Positioning |
Increases systemic vascular resistance and promotes venous return in real-time during symptomatic episodes |
Teach isometric leg contractions, seated leg crossing, and head-of-bed elevation; empower patients with actionable tools for early symptom management |
|
Transcutaneous Vagal Nerve Stimulation |
Modulates autonomic tone by enhancing parasympathetic activity and reducing sympathetic overactivation |
Consider for patients with fatigue, HR variability, or GI dysregulation; low side effect profile; emerging evidence supports use as an adjunct |
|
Vitamin and Nutrient Supplementation |
Corrects deficiencies that impair nervous system function (e.g., B12, D, B6); supports metabolic and neurological integrity |
Monitor labs every 6–12 months; high-dose oral options may be sufficient; reserve parenteral nutrition for patients with severe malabsorption or failure of oral/enteral strategies |
Several drug treatments are used for managing the symptoms of autonomic disorders. Most of these medications are not FDA approved for the use of treating dysautonomias but are used “off-label.” Each of these has been successfully used in treating some patients. Since these medications can produce harmful side effects, patients should take medications only under the supervision of a provider with expertise in the treatment of dysautonomias.
Top 20 Dysautonomia Drugs
| Drug Name/Class | Affects | Notes & Dosing |
|---|---|---|
For Chronic Orthostatic Intolerance |
|
|
|
Midodrine (Proamatine®) Class: alpha-adrenergic agonist |
Primarily works as a vasoconstrictor to increase blood pressure and reduce blood pooling when standing. |
Caution: can cause supine hypertension. (Caution: avoid lying down within 4 hours after dose). One of the few FDA approved drugs for nOH. Recommended Dosing: 10mg PO TID |
|
Fludrocortisone (Florinef®) Class: Mineralocorticoid |
Increases blood volume and blood pressure by increasing fluid reabsorption in the kidneys |
Monitor plasma electrolyte levels, especially potassium. Recommended Dosing: 0.1-0.3 mg PO daily |
|
Desmopressin (dDAVP®) Class: antidiuretic peptide |
Increase blood volume via fluid reabsorption and mild vasoconstrictive effects. Can also reduce frequency and urgency of urination.
|
Only recommended for occasional use; monitor plasma sodium levels. Recommended Dosing: 0.1-0.2 mg PO TID |
|
Droxidopa (Northera®) Class: alpha-beta-adrenergic agonist |
Increases blood pressure via sympathetic stimulation. |
One of the few FDA approved drugs for nOH. Recommended Dosing: 100 – 600 mg PO TID |
|
Propranolol (Ineral®) Class: Nonselective Beta blocker |
Decreases heart rate and blood pressure via sympathetic inhibition. |
Caution: can worsen OI if BP response > HR response. Recommended Dosing: 10-20 mg PO QID |
|
Pyridostigmine (Mestinon®) Class: acetylcholinesterase inhibitor |
Increases blood pressure and muscle strength. |
Caution: may increase gastrointestinal mobility Recommended Dosing: 30-60 mg PO TID |
|
Ivabradine (Corlanor®) Class: HCN channel blocker |
Reduces heart rate. |
Useful in patients with a predisposition to hypotension. Recommended Dosing: 5.0-7.5 mg PO BID |
|
IV Saline /Sodium chloride solution |
Increases blood volume.
(Chronic orthostatic intolerance) |
Non-sustainable therapy: recurrent IV access will eventually lead to damage of venous structures and port placement as an alternative increases the risk of infection. Recommended only as a “rescue” therapy for acute exacerbations. Recommended Dosing: 1-3 L Over 1-3 hours |
For other Dysautonomia Symptoms and Co-Morbidities |
||
|
Clonidine (Catapres®) Guanfacine (Intuniv®) Class: central alpha-2 adrenergic agonist |
Decrease blood pressure and hyperadrenergic response.
Decreasing hyperadrenergic response can lead to improvement in symptoms like insomnia, anxiety, panic attacks and shakiness/tremors.
|
May be associated with rebound tachycardia and hypertension Recommend start at bedtime. Recommended Dosing: 0.05-0.20 mg PO BID |
|
Clonazepam (Klonopin®) Class: benzodiazepine |
Anxiolytic.
Can also reduce BP. |
Recommend starting with a low dose at bedtime. Recommended Dosing: 0.25 – 0.5 mg PO BID-TID PRN |
|
Sertraline (Zoloft®) Class: selective serotonin reuptake inhibitor |
Antidepressant and anxiolytic. |
Caution: initial increase in suicidality risk in children, teens and young adults Recommended Dosing: 50-200 mg PO qd Start 50 mg PO qd, may increase by 25-50 mg/day q wk |
|
Duloxetine Class: selective serotonin and norepinephrine reuptake inhibitor |
Antidepressant and anxiolytic.
Effective agent in treating neuropathic pain and in treating fibromyalgia.
|
Caution: initial increase in suicidality risk in children, teens and young adults Recommended Dosing: 60 mg PO qd |
|
Amphetamines and dextroamphetamine mixed salts (Adderall®) Class: Stimulant |
Increases alertness and cognitive function.
Indirect vasoconstrictor secondary to sympathetic stimulation. |
Reduces appetite. Use with caution as it can be addictive. Monitor for worsening tachycardia. Recommended Dosing: Dosage will depend on the specific stimulant chosen. |
|
Atomoxetine (Strattera®) Class: selective norepinephringe reuptake inhibitor |
Increases attention and reduces brain fog by increasing sympathetic activation. |
Effective in controlled settings but not yet examined in a formal clinical trial with long-term follow-up. Monitor for worsening tachycardia. Recommended Dosing: 80 mg PO daily |
|
Amitriptyline (Elavil®) Class: tricyclic antidepressant |
Antidepressant and anxiolytic. Effective agent in treating neuropathic pain and in treating fibromyalgia.
|
Recommended Dosing: 25 – 100 mg PO qhs Start 25 mg PO qhs and titrate slowly. |
|
Cetirizine (Zyrtec®) Class: H1 antihistamin |
Helps with co-existing MCAS by reducing histamine release and inflammation.
|
Caution: when starting treatment in patients with MCAS, start with ONE drug at a time and slowly add the additional drugs over time. Recommended Dosing: 5 – 10 mg PO qd PRN |
|
Cimetidine Class: H2 antihistamine |
Helps with co-existing MCAS by reducing histamine release and inflammation.
Treats GERD. |
Caution: when starting treatment in patients with MCAS, start with ONE drug at a time and slowly add the additional drugs over time. Recommended Dosing: 1600 mg/day PO divided BID-QID |
|
Cromolyn Class: Mast Cell Stabilizer |
Helps with co-existing MCAS.
Reduces histamine release from mast cells. Can noticeably improve gut inflammation symptoms like bloating, early satiety and abdominal pain.
|
Caution: when starting treatment in patients with MCAS, start with ONE drug at a time and slowly add the additional drugs over time. Recommended Dosing: 200 mg PO QID |
|
Montelukast Class: Leukotriene inhibitors
|
Helps with co-existing MCAS.
Reduces histamine release from mast cells. Can noticeably improve gut inflammation symptoms like bloating, early satiety and abdominal pain. |
Caution: when starting treatment in patients with MCAS, start with ONE drug at a time and slowly add the additional drugs over time. Recommended Dosing: 10 mg PO qd |
|
Bethanechol (Urecholine®) Class: Parasympathomimetic
|
Treats urinary retention. Increases salivation and gut motility. |
Recommended Dosing: 10 – 50 mg PO TID-QID |
|
Gabapentin Class: Anticonvulsant
|
Effective in treating neuropathic pain |
May cause drowsiness or confusion Recommended Dosing: 300 – 1200 mg PO TID |
|
Pregabalin (Lyrica) Class: Anticonvulsant
|
Effective in treating neuropathic pain |
May cause drowsiness or confusion Recommended Dosing: 50-100 mg PO TID |
|
Tramadol Class: partial opioid agonist and SNRI
|
Effective for chronic pain and neuropathic pain |
Recommended Dosing: 50 – 100 mg PO q4-6h PRN |
|
Cyclobenzaprine (Flexeril) Class: Muscle relaxant
|
Can be utilized to treat muscle spasms in EDS patients. Can also be used to treat fibromyalgia.
|
Caution: can exacerbate OI and hypotension Recommended Dosing: Immediate- 5-10 mg PO TID ER- 15 mg PO qd |
Alternative Treatments
TDP strives to bridge the gap between what the top autonomic specialists in the world know and what community providers and patients need to know. TDP is committed to sharing accurate, science-based information and working with the American Autonomic Society (AAS) to make sure our message is scientifically valid, and it gets into the hands of those who need it most. However, we also recognize that some patients access alternative treatments that offer relief from their symptoms. It’s recommended that you talk with your provider about any course of treatment you pursue. Some of these alternative treatments include:
- Acupuncture
- Cranio-sacral massage therapy
- Chiropractor
- Yoga
- Massage therapy
- Eye movement desensitization and reprocessing (EMDR)
- Tap and sound therapy
- Reflexology
- Bemer therapy
- IV therapy
- Hyperbaric oxygen change
- Deep breathing exercises
- Dry brushing
- Alternative diets: You may consider an organic, whole foods approach that reduces sugar, certain carbohydrates, and artificial/processed foods. Gluten and dairy free diets may help some people.
Prognosis
No two dysautonomia patients look the same. Dysautonomia can be mild or debilitating. A more severe case will require significant lifestyle changes as you try different treatments to address symptoms. For some patients, the goal is to have more good days than bad. Symptom management is possible, but it takes time and patience. Because the autonomic nervous system adapts and changes, the course of your condition may change as well. Some patients find a treatment plan that works for a while, but then a new symptom appears and becomes their chief complaint. This is why finding a provider who understands dysautonomia and can help you manage your individual case is so important. It’s also why patients must become their own advocate and participate in the process of managing their symptoms. This includes partnering with your doctor by tracking symptoms, responses to treatment, and providing this data at your appointments.
Practical Tips for Living with Dysautonomia
- Energy drinks and alcohol should be consumed with caution or avoided. Both are dehydrating in nature and can affect the heart and nervous system. Carbonated beverages should be ingested sparingly, or not at all, as the body must work to expel the extra ingested carbon dioxide.
- Eat smaller meals to aid digestion
- Avoid standing or sitting for long periods of time. If you feel dizzy, sit down, lie down, and raise your feet.
- Avoid heat. This includes hot showers.
- Get enough sleep. Establish an evening routine and try to stick to it. This is especially important for teens with POTS.
- Manage stress
- Ask for help when you need it
- Pay attention to your mental health and ask for help when you need it.
There may not be a cure, but there is hope as you take ownership of your healthcare and work with your provider on finding treatments that help decrease your most difficult symptoms. It takes time and diligence, but it’s possible to increase the number of good hours, days, weeks, and years.
